Overview
The ulnar nerve (ventral rami C8-T1) supplies the
majority of intrinsic hand muscles and two forearm muscles. This contrasts with
the median nerve, which mainly supplies the forearm. The ulnar nerve ay be
compressed at several points along its course.
Gross Anatomy
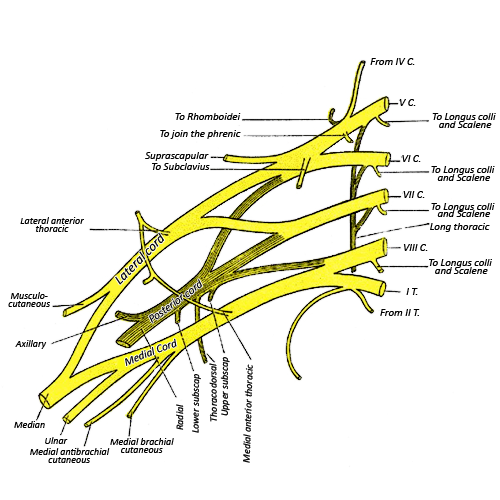
The ulnar nerve is a terminal branch of the medial cord of the brachial plexus.
The nerve descends down the medial side of the arm, and first passes through the arcade of Struthers, a band of fascia connecting the medial intermuscular septum and the medial head of the triceps. The nerve then passes through the cubital tunnel, where the ulnar nerve takes a very superficial course when it passes behind the medial epicondyle. The nerve lies directly under the skin, and knocking one’s elbow results in a tingling in the nerve’s distribution. Hence the term ‘funny bone’. The nerve then emerges between the two heads of flexor carpi ulnaris (which it innervates), and gives branches to the ulnar head of flexor digitorum profundus. It descends down the forearm, deep to the flexor carpi ulnaris, medial to the ulnar artery, until it reaches Guyon’s canal at the wrist. This is a narrow tunnel through which the ulnar nerve and artery enter the hand. It is bordered by the pisiform and pisohamate ligament on the ulnar side, and the hook of hamate on the radial side. The hypothenar muscles and the flexor retinaculum form the floor. The palmar carpal ligament forms the roof.
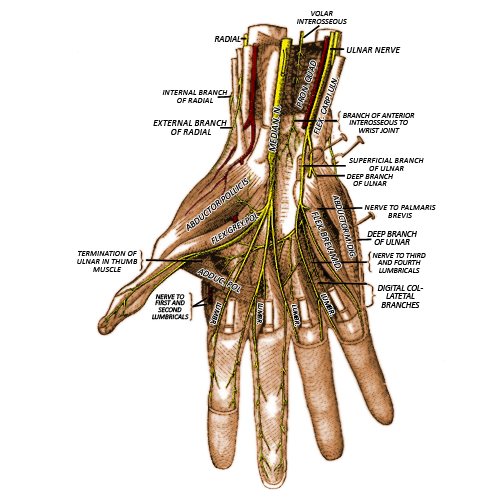
At the wrist it divides into a motor and
sensory branch. The sensory branch further divides into a palmar and dorsal
cutaneous nerve that supplies sensation to the ulnar one and half fingers on
the palmar and dorsal side. The motor branch supplies all the interossei (4
dorsal and 3 palmar), the ulnar two lumbricals (four in total), and adductor pollicis
brevis.
Clinical Anatomy
Injury to the ulna nerve can lead to
a clinical sign known as the “ulna claw”.
For example traumatic injury to the
ulna border of the proximal forearm may injure the nerve.
This may result in denervation to
several muscle groups, most importantly;
1.
Lumbricals to the little and ring
finger resulting in an inability to flex the fingers at the MCPJ
2.
The FDP of the ring and little finger
resulting in an inability to flex the fingers at the DIPJ
As a consequence the unopposed action
of the long extensors of the MCPJ results in hyperextension at this joint. If the ulna
portion of FDP is also injured the DIPJ will not flex, resulting in a mild
claw. However if the FDP is not denervated, e.g. following an injury at the
wrist, the FDP will continue to function resulting in a more prominent claw.
Quick Anatomy
Key Facts
Developmental precursor- Alar and basal
plate of C8,T1 spinal nerves
Origin- C8,T1
Branches- motor branch, dorsal cutaneous
branch, palmar cutaneous branch.
Muscles supplied- flexor carpi ulnaris,
ulnar part of flexor digitorum profundus, interossei, ulnar two lumbricals.
Dermatome- Ulnar one and a half fingers and palm on
the palmar and dorsal surface of the hand.
Aide-Memoire
Summary
The Ulnar nerve supplies the flexor carpi ulnaris and
supplies the ulnar head of flexor digitorum profundus. It also supplies the
majority of intrinsic hand muscles, and sensation to the ulnar one and a half
fingers and palm on the palmar and dorsal side.