Overview
Gross Anatomy
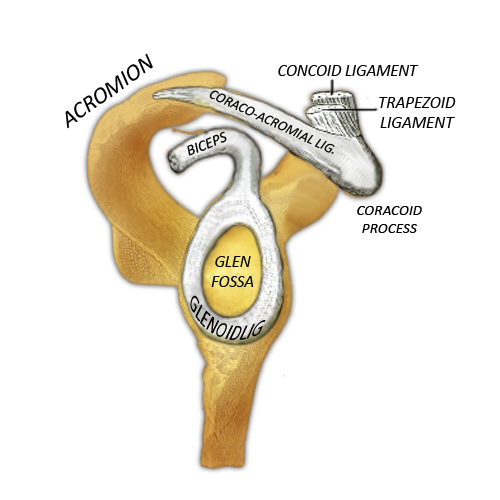
The pear shaped glenoid fossa arises from the superior lateral surface of the scapula. This shallow and dish like fossa is deepened by the glenoid labrum, which is a fibrocartilaginous ring that surrounds the edge of the fossa. It articulates with the globe shaped head of the humerus.
Joint capsule
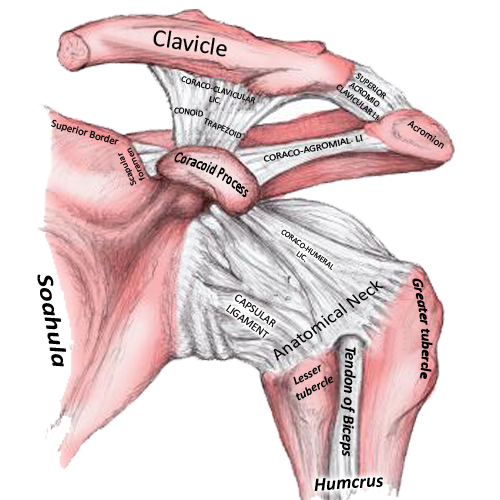
The fibrous joint capsule attaches to the margin of the glenoid cavity and passes across to the anatomical neck of the humerus. The joint capsule is relatively slack inferiorly, in order to allow shoulder elevation. It has two openings; one between the tubercles of the humerus for the long head of biceps, the other anterior and inferior to the coracoid process for the subscapular bursa. This is lined by the synovial membrane.
The inherent instability of the joint is balanced by the large number of supportive ligaments and muscles to reduce the likelihood of dislocation. These stabilising structures are grouped into static and dynamic stabilisers. Static stabilisers include the anatomical congruity, glenoid labrum (deepens the glenoid fossa and provides some negative suction effect), the joint capsule, coracohumeral ligaments and glenohumeral ligaments.
The glenohumeral and coracohumeral ligaments
There are three glenohumeral ligaments, superior, middle and inferior. These are thickenings of the capsule. The superior ligament prevents inferior translation of the humeral head when the arm is fully adducted. The middle ligament resists anterior and posterior translation when the shoulder is in mid range abduction. The inferior ligament is divided into anterior, posterior and superior bands. The anterior band resists posterior distraction of the humeral head when the shoulder is flexed and internally rotated. The inferior part of the inferior ligament resists anterior and inferior translation when the arm is abducted to 90 degrees. The superior band provides static stability.
The coracohumeral ligament is a strong band passing from the coracoid process to the anterior aspect of the base of the coracoid and limits posterior dislocation in a flexed adducted and internally rotated shoulder.
The coracoacromial arch
This structure is formed by the coracoid process, coracoacromial ligament and acromion. It is very strong and prevents superior displacement of the humeral head from the glenoid cavity.
Muscles
Several muscles act on the shoulder joint and allow movement in multiple planes. A group of four muscles which pass from the scapular to the proximal humerus, form a sheath of tendons across the joint known as the "rotator cuff". These provide dynamic restraints which pull the head of the humerus into the glenoid fossa in various positions and planes of motion. They are summarised in the table below;
The long head of biceps depresses the humeral head into the glenoid fossa. The joint allows for elevation of the shoulder up to 90 degrees, after which scapular rotation i.e. elevation is required for further abduction.
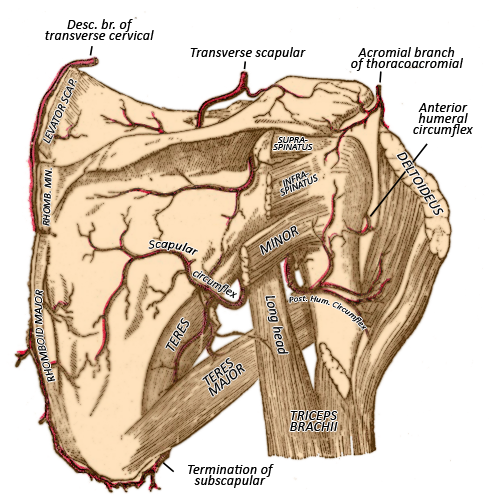
Blood supply
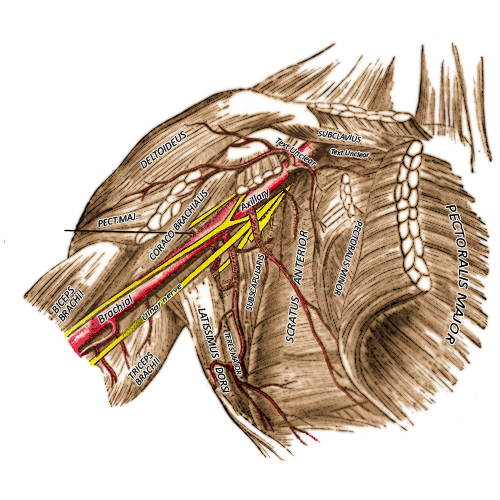
The ascending branch of the anterior humeral circumflex, and the posterior humeral circumflex supply the shoulder joint. These arise from the axillary artery.
Bursa
There are numerous bursae that surround including the subacromial (beneath the acromial arch), the subdeltoid (deep to the deltoid muscle, subscapular (between the subscapularis tendon and neck of the glenoid fossa) and subcoracoid (beneath the coracoid process). The subacromial and subscapular bursae are the most common sites of bursitis.
Clinical Anatomy
Shoulder pain is common; it affects 16-24% of people
and is the third most common musculoskeletal complaint seen in general
practice. Accurate diagnosis can be difficult due to the complexity of the
glenohumerual joint complex.
Subacromial impingement syndrome develops as tissue
underneath the acromion becomes inflamed due to irritation of the bursa or
rotator cuff as repetitive movement occurs in the confined space.
Rotator cuff tears are common, particularly in the
elderly. 25% of 60 year olds will have a tear, this rises to 50% at 80 years. MRI
arthrogram is the gold standard for diagnosis.
Adhesive capsulitis, most commonly affects women
over 40 years. It is associated with diabetes, immobilisation (for example
after a subacromial decompression!), trauma and thyroid pathology. Patients are
most commonly restricted in abduction and external rotation. The disease
follows three main stages; freezing, frozen and thawing, which typically last
for 12-24 months in total.
Quick Anatomy
Key Facts
Developmental precursor- Limb bud, somatic layer of lateral mesoderm
Blood supply-
Anterior and posterior humeral circumflex arteries
Nerve supply-
Articular branches of the suprascapular, subscapular, axillary and musculocutaneous
nerves.
Bursae-
Subacromial, subcoracoid, subscapular, subdeltoid.
Aide-Memoire
Always remember the blood supply to
the joint is from the anterior and posterior circumflex arteries
TISS- an acronym to remember the
rotator cuff muscle (teres minor, infraspinatus, supraspinatus and
subscapularis).
Summary
The
glenohumeral joint is also known as the shoulder joint. It is formed between
the glenoid fossa of the scapula, and the head of the humerus. It is a
relatively unstable joint and has static and dynamic support.
References
Dinnes J, Loveman E,
McIntyre L, et al. The effectiveness of diagnostic tests for the assessment of
shoulder pain due to soft tissue disorders: a systematic review. 2003. In: NIHR
Health Technology Assessment programme: Executive Summaries. Southampton (UK):
NIHR Journals Library; 2003-. Available from:
https://www.ncbi.nlm.nih.gov/books/NBK62241
Saulle,
M. & Gellhorn, A.C. Curr Phys Med Rehabil Rep (2017) 5: 1.
https://doi.org/10.1007/s40141-017-0149-6