Overview
Gross Anatomy
Articular structure

Actions
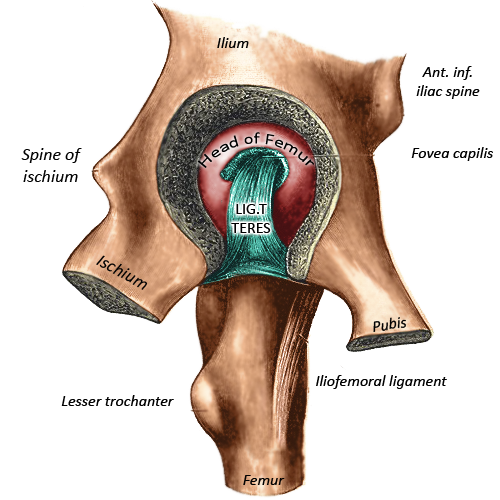
Blood supply
Nerve Supply
“the nerve supplying
a joint supplies also the muscles which move the joint and the skin covering
the articular insertion of those muscles”(7).
Development
Clinical Anatomy
Femoral neck fractures
Hip
fractures represent a significant public health burden with around
70,000-75,000 cases a year with an estimated cost of £2 billion per a year, 10% of cases die
within one month and a third die within 12 months(10). This is a marker of the
complex co-morbidities of these patients, thus a thorough history into the
cause of the fall needs to be undertaken and all patients should be managed
within a multi-disciplinary environment with orthogeriatric input.
Management
is nearly exclusively surgical with NICE recommending surgery on the day or day
after admission with rapid correction or control of manageable co-morbidities
to facility surgery(10).
Surgical
options depend on the type of fracture. Firstly one must deduce if the fracture
is intra or extra-capsular. In extra-capsular fractures blood supply to the
femoral head is preserved and not threatened. If the fracture is above or
including the lesser trochanter extramedullary fixation such as a sliding hip
screw should be used, if subtrochanteric intramedullary fixation is advisable(10).
Intracapsular
fractures are more complex. Due to the blood supply, as described above, the
viability of the femoral head is threatened and avascular necrosis may occur.
Fixation technique decision is dependent on the degree of displacement.
Displacement is judged on plain film radiographs with both AP and lateral views
assessed. Gardens classification is used to classify femoral neck fractures.
Non displaced fractures (Gardners I and II) undergo fixation with cancellous
scews or sliding hip screw. Displaced fractures (Gardners III and IV) require
arthroplasty due to disruption of the blood and high risk of avascular necrosis
, this can be total hip replacement or hemiarthroplasty(10). Indications for total hip
replacement are defined by NICE as the following:
· Were able to walk
independently out of doors with no more than the use of a stick and
· Are not cognitively
impaired and
· Are medically fit for
anaesthesia and the procedure
Post
operatively early mobilization is the aim with multi-disciplinary
rehabilitation and future falls prevention.
Osteoarthritis
Pain
secondary to osteoarthritis of the hip joint is present in 12% of adults of 65
years and above(11). Osteoarthritis of the hip may
be primary or secondary to previous infection, injury or disease.
Osteoarthritis of the hip joint has a worse prognosis than that of the hand or
knee with a significant proportion requiring operative management at five years(11).
Pain
is often the primary complaint, this can be felt in the anterior groin or it
can be more generalized over the buttock and down to the knee. Patients may
well complain that they find it hard to put on their shoes or cut their toe
nails. Key signs on examination are an antalgic gait, muscle wasting,
painful/reduced range of motion (internal rotation is the first effected), in
later stages a fixed flexion deformity can be found(11).
Diagnosis
can be made clinically, however AP plain film radiographs of the pelvis may
well be useful.
Treatment
should be individualized to patient factors. Education, strengthening with
physiotherapy input, weight loss (if required), activity modification and
assistive devices should be provided. Alongside this appropriate analgesia is
needed. This should initially be paracetamol +/- non-steroidal
anti-inflammatory drugs (NSAIDs). If prescribing a NSAID a proton-pump
inhibitor should be co-prescribed and NSAIDs are not suitable/appropriate for
all patients. Some may add weak opioids such as codeine however the evidence
for this is poor(11). Intra-articular injection can
also be considered; this may also provide diagnostic information.
If
a patient continues to suffer from significant symptoms and pain operative
intervention may be considered. Surgical options consist of arthroscopy,
osteotomy, hip resurfacing and replacement(12). Patients age and degree of
arthritic changes are key factors in the decision making process.
Developmental dysplasia of the
hip (DDH)
DDH
is a spectrum of disease ranging from mild dysplasia of the acetabulum to
irreducible dislocation. 1-1.5 in 1000 live births are affected and it is more
common in female patients, breech presentation and intra-uterine overcrowding(13,
14). The left hip is
more commonly affected(13,
14).
In
the neonate DDH is asymptomatic and therefore is screened for with Barlow and
Ortolani tests. After the age of around 3 months the tissues begin to tighten
and the aforementioned tests become unreliable, signs at this stage will be
loss of abduction, apparent shortening of the thigh (Galeazzi sign) and
asymmetrical skinfolds (however may be present in normal individuals)(13). After the child begins to walk
other signs such as a trandelenburg gait and leg-length discrepancy will become
apparent.
Ultrasonography
prior to femoral head ossification (4-6 months) and plain film radiographs
after ossification are the mainstay of investigation(13,
14).
Treatment
depends on the age of diagnosis. Ultimately the aim is to maintain a reduced hip
joint providing the optimal environment for normal hip development. As age at
diagnosis increases this is harder to achieve, potential for hip remodeling
reduces and more complex treatments are required. The following gives an overview
of treatment options available according to age(13-15):
Under 6 months
· Splintage usually
with a Pavlik harness
· Monitor with USS
6 months to 18 months
· Closed reduction (+/-
adductor tenotomy)
o If difficulty in
reduction consider arthrogram to assess if soft tissue is blocking reduction
· If closed reduction
fails open reduction
· Reduction (closed or
open) is held with a hip spica cast
18 months to 3 years
· Open reduction (+/-
osteotomy)
3 to 8 years
· Open reduction and
osteotomy
Over 8 years
· Can be treated
non-surgically or with osteotomy
· Irrespective of above
management choice must plan for a total hip replacement in adult life
Quick Anatomy
Key Facts
Development: Derived from the
mesoderm.
Blood
supply: Retinacular vessels (branches of the
circumflex vessels) are the predominant blood supply for the femoral head.
Branches of the internal iliac artery supply the acetabulum.
Nerve
supply: Innervation of the hip joint is from the
femoral, obturator, sciatic nerve, superior gluteal and nerve to the quadratus
femoris.
Aide-Memoire
Summary
The hip joint is a major load bearing ball
and socket joint connecting the pelvis to the lower limb. The joint is very
stable but retains multi-axial movement. Pathological processes can occur in
all stages of life and may well require surgical intervention.
References
1 Weber E, Ritting A. Normal Hip Embryology and
Development. In: Berry D, Lieberman J, editors. Surgery of the Hip. 1 ed:
Elsvier Health Sciences; 2012. p. 200-5.
2 Wheeless C. Embryology of the Hip. In:
Wheeless C, editor. Wheeless' Textbook of Orthopaedics: Duke Orthopaedics;
2013.
3 Moore KL, Dalley AF, II, Agur AMR.
Clinically oriented anatomy. 5th ed. ed. Philadelphia, Pa. ; London: Lippincott
Williams & Wilkins; 2006.
4 Moses K, Banks J, Nava P, Petersen D. Hip
Joint. In: Moses K, Banks J, Nava P, Petersen D, editors. Atlas of clinical
gross anatomy. 2nd ed. Philadelphia, PA: Elsevier/Saunders; 2013. p. 512-25.
5 Hoffmann R, Haas N. Fractures of the
femoral neck (31-B). [cited 2016
10/3/16]; Available from: https://www2.aofoundation.org/wps/portal/!ut/p/a0/04_Sj9CPykssy0xPLMnMz0vMAfGjzOKN_A0M3D2DDbz9_UMMDRyDXQ3dw9wMDAx8jfULsh0VAdAsNSU!/?bone=Femur&segment=Proximal&soloState=lyteframe&contentUrl=srg/popup/further_reading/PFxM2/31/661_31_fem_neck_fxs_gen_consid.jsp
6 Itokazu M, Takahashi K, Matsunaga T, et
al. A study of the arterial supply of the human acetabulum using a corrosion
casting method. Clin Anat. 1997;10(2):77-81.
7 Hilton law. Farlex Partner Medical Dictionary; 2012.
8 Birnbaum K, Prescher A, Hessler S, Heller
KD. The sensory innervation of the hip joint--an anatomical study. Surg Radiol
Anat. 1997;19(6):371-5.
9 Cheatham SW, Kolber MJ. Orthopedic
management of the hip and pelvis. St. Louis, Missouri: Elsevier, Inc.; 2016.
10 NICE. Hip fracture: management. National
Institute for Health and Excellence Guidance. 2011 22/06/11.
11 NICE. Osteoarthritis. Clinical Knowledge
Summaries. 2015.
12 Gandhi R, Perruccio AV, Mahomed NN.
Surgical management of hip osteoarthritis. CMAJ. 2014 Mar 18;186(5):347-55.
13 Sankar W, Horn D, Wells L, Dormans J.
The Hip. In: Kliegman R, Behrman RE, Nelson WE, editors. Nelson textbook of
pediatrics. Edition 20 ed. Phialdelphia, PA: Elsevier; 2016. p. 3274-83.
14 Schmitz M, Rush J, Milbrandt T.
Pediatric Orthopaedics. Miller's review
of orthopaedics. Seventh edition. ed. Philadelphia, PA: Elsevier; 2016. p.
264-334.
15
Chalmers CR, Smith CP. MRCS A essential revision notes. Knutsford: PasTest;
2012.